
, Bridge Magazine , Health Articles
Margaret Wilson worked at a Nurse Continence Specialist- led pessary clinic in a rural service, and provides women with advice and reassurance. At the clinic, specially trained nurses see women who are usually referred by their GP for pelvic muscle assessment and to be fitted for a pessary.

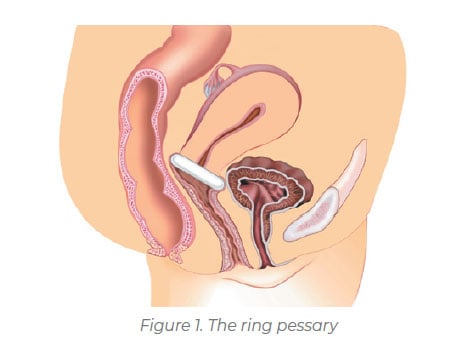
Margaret, who now works on the National Continence Helpline (NCHL), says pessaries have had a resurgence in popularity as they are currently made from silicone and are easier to self-manage and insert. “We usually start with a ring pessary, a removable silicone device which is inserted into the vagina like a tampon.” (See Figure 1).
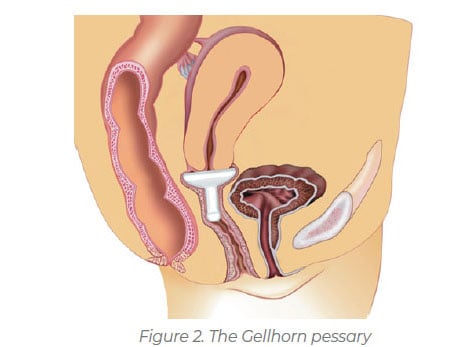
If the ring pessary is not strong enough to hold back a prolapse, women can progress to a ‘Gellhorn’ pessary, a stronger device designed to hold back any prolapsed tissue. (See Figure 2).
Another type of pessary, often used to manage third-degree uterine prolapse, is the cube pessary. This is a more supportive pessary for the uterus, particularly if there is a loss of vaginal tone. For women with incontinence when they laugh, cough, sneeze or exercise, a dish pessary or a ring with a knob is recommended. This type of pessary puts pressure on or supports the urethra, preventing urine leakage.
Once a pessary is inserted and fitted properly, most women won’t know it’s there and should experience immediate improvement. In the clinic, once women were fitted with their pessary, they were encouraged to walk, go up a flight of stairs, squat and sit on the toilet all as normal. If properly fitted, the pessary will not fall out and women are encouraged to keep doing their pelvic floor exercises to strengthen these muscles.
When is a pessary not recommended?
- When there is vaginal irritation or infection
- When severe arthritis may compromise the ability to self-manage, insert and remove the pessary
- When there is declining memory or dementia, so that the pessary is forgotten and not checked regularly, unless the person has reliable care
- When a person is at risk of neglecting to attend follow up appointments.
Remember, regular check-ups are necessary. If the pessary is left in the vagina for long periods of time it may become embedded as the vaginal tissue grows around it. Good education is vital around proper insertion, removal, care, and cleaning, and reduces the risk of complications.
For more information on finding a Pelvic Floor Physiotherapist or Nurse Continence Specialist in your area, contact the National Continence Helpline on 1800 33 00 66.
Margarets Key tips
✔ Get checked regularly. After the pessary is first inserted it should ideally be checked a fortnight later, then monthly and every 6 to 12 months to ensure healthy vaginal tissues.
✔ Remove the pessary overnight at least once a week to allow the vaginal tissues to rest (note: a cube pessary needs to be removed daily).
✔ Most styles of pessaries are safe to leave in during menstruation, however, need to be washed daily.
✔ post-menopausal women will usually need vaginal oestrogen for at least 6 weeks before a pessary is fitted to ensure comfort and the vaginal tissue is thick and well lubricated to prevent irritation.
Get Support
Phone the free National Continence Helpline 1800 33 00 66 to speak to a nurse continence specialist about bladder and bowel health.
This story was first published in Bridge Magazine. Subscribe and receive Bridge straight to your inbox.